Guest editor: Mireia Jofre-Bonet | VP & Head of Research
|
|
|
|
|
Ignoring the needs of our future workforce could have disastrous consequences for the UK NHS and its patients. In economics, we have a pretty complicated name (hyperbolic discounting) for a very common human inclination, that is to consider that today matters much more than tomorrow. However, the UK NHS is facing the consequences of the workforce being planned mostly for the short term as if tomorrow doesn’t quite count.
|
|
|
In the aftermath of COVID-19, more ordinary concerns are recapturing our attention. We are slowly leaving behind a constant state of emergency and, at times, unavoidable improvisation.
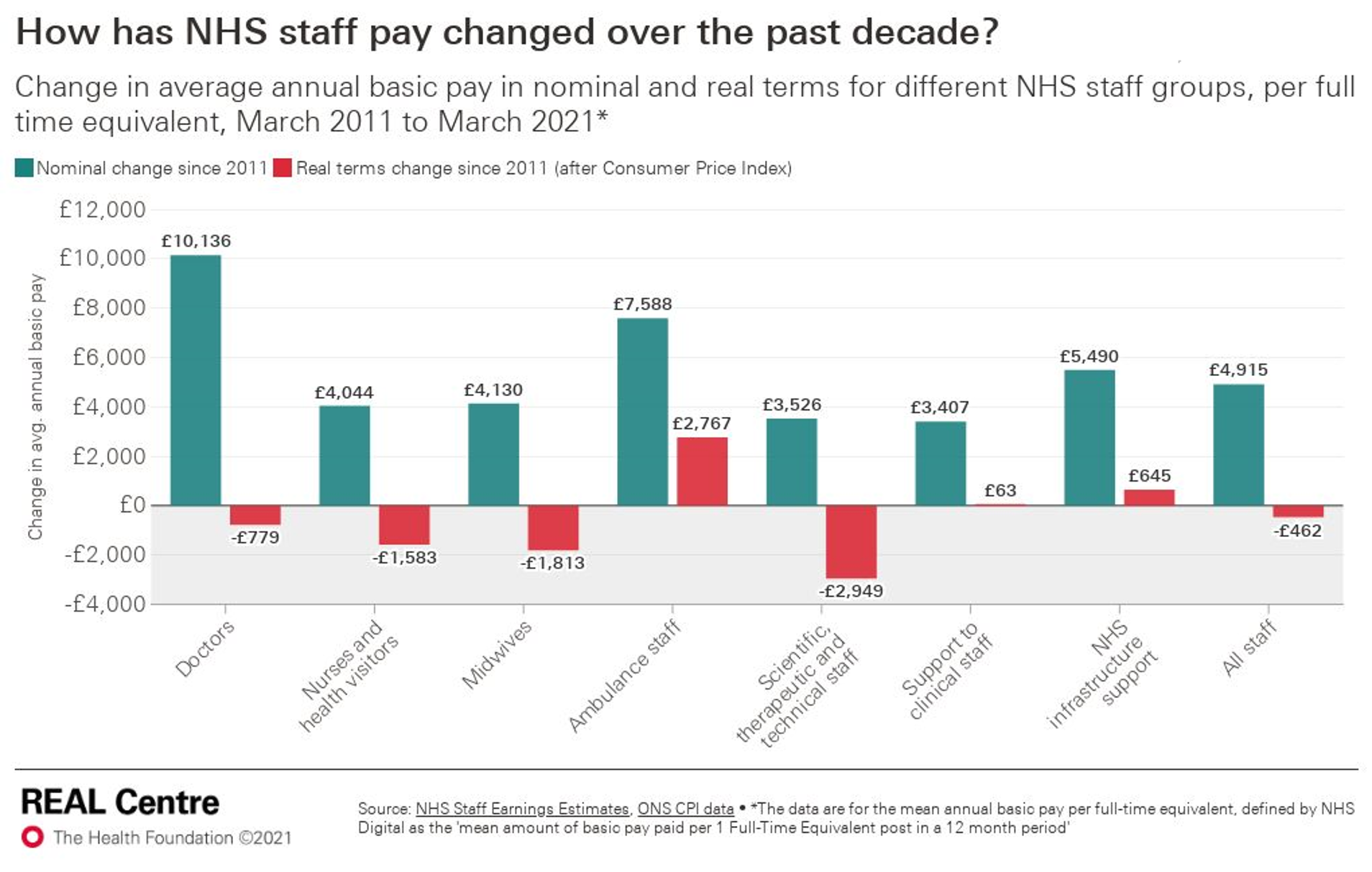
Sadly, after the heroic effort of the NHS staff during the pandemic, the future of the NHS looks increasingly bleak: in 2021, at least 20% of its staff were considering early retirement or switching careers. Being overworked by clinical and escalating administrative tasks and the lack of incentives and rewards explain the looming NHS staff exodus. Focusing on the lack of incentives for retention, the below graph reveals how medical staff have suffered real wage losses in the last decade.
The resulting number of vacancies is astonishingly high. NHS England alone had 110,192 vacancies, equivalent to an 8.3 % vacancy rate at the end of 2021. GPs are experiencing a similar situation, and certain medical specialities are under higher pressure than others (i.e., anaesthetists or radiologists). There is no sign that these vacancies are going to be filled in the near future. Welcome, but insufficient, piecemeal governmental efforts to increase nurses, doctors and GP recruitment and the partial restitution of the nurses’ and medical bursaries are not considered enough to address the present and future staffing problems.
The UK NHS workforce shortages issue is not new; it has been brewing for years and is largely the result of the lack of workforce long-term planning during the last decade, which the COVID-19 crisis compounded.
Safe and efficient levels of staffing tomorrow require adjusting medical staff training and education many years in advance. In an effort to take a step in the right direction, the government merged Health Education with NHS England and NHS Improvement, but this has yet to result in a long-term plan by which the latter can inform the training needs to be implemented by the former.
The looming NHS workforce cataclysm has caused a compelling outcry from a broad range of experts and analysts, such as The Kings Fund, The Health Foundation, and Nuffield Trust, to name only a few. It is also the object of attention of numerous news outlets (the British Medical Journal, Health Services Journal, The Economist, The Times, The Guardian, The Independent, etc.). Furthermore, an amendment to the Health and Care Bill calling for an objective and independent mechanism to predict the future right staffing of the NHS received the support of over 100 organisations, but it failed to be incorporated in the approved Act.
In conclusion, COVID-19 has made it more evident than ever that a health care system must be resilient as well as sustainable. These two objectives might clash at times, but this is escalated when the budget is guided by short-term objectives that do not take into consideration the needs of tomorrow. Given the eternal budgetary constraints faced by the NHS, understanding the health care system workforce’s upcoming requirements are more vital than ever. Carefully orchestrated integration and coordination solutions could alleviate today and tomorrow’s blockages. It is time that decision-makers realise the benefits of behaving maturely, stop ignoring the future, and leave behind the current short-sighted approach to NHS workforce planning.
|
|
|
“Despite a proud history of medical discovery and innovation, the NHS has difficulty adopting and spreading new treatments [...] Compared to similar countries, the UK adopts just 20 per cent of NICE approved medicines within 12 months of approval”.
|
|
|
This report published by the Institute for Public Policy Research, a British think tank, shows that across clinical priorities, access is poor, outcomes are below international standards and inequalities are widening. Clinical areas with declining access to and
|
|
quality of care include mental health, dementia and other long-term conditions. There is a risk that more people with an ability to pay will supplement public health care with paid-for products, leading to a dual health system and increased inequalities.
|
|
|
NICE’s new evaluation manual replaces the End of Life (EOL) criteria with a severity modifier. The new modifier is arguably an improvement over EOL because it defines severity more broadly. However, the same type of criticism applies to the new modifier: there is little evidence indicating that it aligns with societal preferences. This blog outlines the new modifier and discusses the need for further related research.
|
|
Following an ISPOR session, two panellists compare the value assessments of digital health technologies (DHTs) in England and Germany. In England, NICE has focused on testing its methods for assessing DHTs and has published guidance on two technologies. Germany’s focus is more on the outpatient setting and its progress has resulted in the assessment and listing of 28 DHTs in less than a year.
|
|
Despite open source models (OSMs) could increase the transparency, credibility, and reuse of models, the number of OSMs remains low. This survey conducted with ISPOR members confirms the potential benefits of OSMs and highlights several barriers that hamper their widespread adoption. Fundamental changes are needed across the research community if OSMs are to become widely adopted.
|
|
|
An increase in the total number of referrals for suspected cancer has been observed since February last year, going from 2.4 million before the pandemic to 2.7 million. However, the proportion of patients seen within the two-week benchmark of waiting time is at record low: 83% compared to 91% before the pandemic.
|
|
The Paper presents an analysis of the potential risks and benefits of reforms seeking to strengthen evidence on orphan drugs and to ensure that adequate incentives for orphan drug development are coupled to a more sustainable long-term trajectory for orphan drug pricing. Among the reforms analysed there are outcome-based contracts and indication-based pricing.
.
|
|
In 2015, the Food and Drug Administration (FDA) launched a five-year action plan aimed at improving diversity in clinical trials. Despite this, Black patients remained inadequately represented in clinical trials for medicines, with a median of one-third the enrolment that would be required. Fewer than 20% of medicines had data regarding treatment benefits or side effects reported for Black patients; neither measure improved during the action plan period.
|
|
|
18 MAY | In celebration of our 60th anniversary, we invite you to join us for a seminar where we are considering the Past, Present, and Future of Health Economics followed by a rooftop drinks reception in Washington, D.C. Tickets are free but limited.
Book your free ticket today.
|
|
26 MAY | Join us for the first OHE Masterclass of 2022 where thought leaders and international expert will discuss theory, practice and current policy debate around severity.
Book your ticket today for our Early Bird discount.
Book your ticket.
|
|
ON-DEMAND | We have launched a new suite of on-demand lectures, associated with our Masterclass Series, which are available on a mix-and-match basis for only £20 each.
To get you started on your learning journey, we are offering the first ‘What is Value?’ lecture for free.
View all available lectures.
|
|
|
|